Ebola Virus: Symptoms, Diagnosis, Treatment and Care
Author: Disabled World (DW)
Updated/Revised Date: 30 Jul 2026
Table of Contents:
Synopsis - Definition - About This Section - FAQs - Publications - Subtopics
Synopsis
Information on the Ebola virus, including transmission facts, signs and symptoms, diagnosis, and current treatment and prevention methods for the disease.
At a Glance
- 1 - The first Ebola virus species was identified in 1976 near the Ebola River in what is now the Democratic Republic of the Congo, with bats considered the most likely natural reservoir host.
- 2 - Symptoms can appear 2 to 21 days after exposure, usually within 8 to 10 days, and humans are not infectious until symptoms develop.
- 3 - The average case fatality rate is around 50 percent, though past outbreaks have ranged from 25 to 90 percent, and standard care remains limited to supportive therapy.
Topic Definition
- Ebola Virus Disease
Ebola virus disease (EVD), also known as Ebola hemorrhagic fever or simply Ebola, is a severe and often fatal illness affecting humans and other primates, caused by viruses of the family Filoviridae, genus Ebolavirus. The virus passes to people from wild animals and then spreads through human-to-human transmission, typically by direct contact with the blood or secretions of an infected person or with contaminated objects such as needles. After an incubation period of two days to three weeks, it generally begins with fever, sore throat, muscle pain, and headache, followed by vomiting, diarrhea, rash, reduced liver and kidney function, and in some cases internal and external bleeding. Of the five identified subspecies, four have caused disease in people, making Ebola one of the deadliest viruses known to humankind.
Overview
Ebola virus disease (EVD; also Ebola hemorrhagic fever, or EHF), or simply Ebola, is a disease of humans and other primates caused by Ebola viruses. The virus is transmitted to people from wild animals and spreads in the human population through human-to-human transmission. Signs and symptoms typically start between two days and three weeks after contracting the virus with a fever, sore throat, muscle pain, and headaches. Then, vomiting, diarrhea and rash usually follow, along with decreased function of the liver and kidneys. At this time, some people begin to bleed, both internally and externally. Ebola hemorrhagic fever is one of a number of Viral Hemorrhagic Fevers. It is a severe and many times fatal disease in people and non-human primates such as gorillas, chimpanzees, and monkeys. Ebola HF is caused by infection with a virus of the family, 'Filoviridae' genus Ebola-virus. When an infection happens, symptoms usually start quickly.
The first Ebola virus species was discovered in the year 1976 in what has become the Democratic Republic of the Congo, near the Ebola River. Since that time, outbreaks have appeared sporadically. The Ministries of Health (MoH) of both Liberia and Guinea and the World Health Organization (WHO) have reported an outbreak of Ebola HF in several Liberian and Guinean districts.
There are 5 identified subspecies of Ebola-virus. 4 of the 5 have caused disease in people:
- Ebola virus
- Sudan virus
- Tai Forest virus
- Bundibugyo virus
The 5th subspecies, Reston virus, has caused disease in non-human primates, but not in people.
The natural reservoir host of Ebola viruses is something that remains unknown at this time. Based on available evidence and the nature of similar viruses; however, researchers believe the virus is, 'zoonotic,' or, 'animal-borne,' with bats being the most likely reservoir. 4 of the 5 subtypes happen in an animal host native to the continent of Africa.
A host of similar species is most likely associated with Reston virus, which was isolated from infected cynomolgous monkeys imported to America and Italy from the Philippines. Several workers in the Philippines and in American holding facility outbreaks became infected with the virus, yet did not become sick.
Transmission
Because the natural reservoir of Ebola viruses has yet to be proven, the manner in which the virus first appears in a person at the beginning of an outbreak remains unknown. Researchers; however, have hypothesized that the first person becomes infected through contact with an infected animal. When an infection does happen in people, there are various ways in which the virus may be transmitted to others. These ways may include direct contact with the blood or secretions of a person who is infected, or exposure to objects such as needles that have become contaminated with infected secretions.
The viruses that cause Ebola HF are many times spread through family members and friends because they come in close contact with infectious secretions while caring for sick others. During outbreaks of Ebola HF, the disease spreads rapidly within healthcare settings, such as in hospitals or clinics. Exposure to Ebola viruses may happen in healthcare settings where staff members are not wearing appropriate protective gear such as gloves, gowns, and masks.
Proper cleaning and disposal of instruments such as syringes and needles is important. If instruments are not disposable, they need to be sterilized before they are used again. Without adequate sterilization of these instruments, virus transmission might continue and amplify the outbreak.
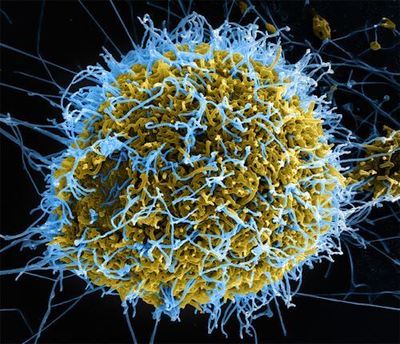
A digitally colorized scanning electron micrograph (SEM) depicts filamentous Ebola virus particles (blue) budding from a chronically infected VERO E6 cell (yellow-green). Photo: National Institute of Allergy and Infectious Diseases, via the Centers for Disease Control and Prevention.
Signs and Symptoms of Ebola
Several symptoms of Ebola HF exist. The symptoms may appear anywhere from 2-21 days after a person is exposed to Ebola viruses. People usually experience symptoms within 8-10 days. Symptoms of Ebola HF May Include:
- Fever
- Cough
- A Rash
- Hiccups
- Diarrhea
- Vomiting
- Red Eyes
- Headache
- Weakness
- Chest pain
- Sore throat
- Stomach pain
- Lack of appetite
- Difficulty breathing
- Difficulty swallowing
- Joint and muscle aches
- Bleeding inside and outside the body
Some people who become sick with Ebola HF do recover; other people do not. The reasons why are not fully understood. It is known; however, that people who die from Ebola HF typically do not develop a significant immune response to the virus at the time of their death.
Diagnosis
Diagnosing Ebola HF in a person who has become infected for only a few days is hard because the early symptoms, such as a skin rash and red eyes, are non-specific to Ebola virus infection and are often times seen in people with more common diseases. If a person presents with early symptoms of Ebola HF; however, and there is reason to believe that Ebola HF should be considered, the person should be isolated, and public health professionals should be notified. Samples from the person may then be collected and tested to confirm the infection.
Treating Ebola
The standard treatment for Ebola HF remains limited to supportive therapy. The therapy consists of balancing the person's electrolytes and fluids, maintaining their oxygen status and blood pressure, as well as treating them for any complicating infections. Timely treatment of Ebola HF is important yet challenging because the disease is hard to diagnose clinically in the early stages of infection. Early symptoms such as fever and headache are non-specific to Ebola virus, and infection might be initially misdiagnosed.
Ebola Virus Contact Tracing
Contact tracing is finding everyone who comes in direct contact with a sick Ebola patient. Contacts are watched for signs of illness for 21 days from the last day they came in contact with the Ebola patient. If the contact develops a fever or other Ebola symptoms, they are immediately isolated, tested, provided care, and the cycle starts again, all the new patient's contacts are found and watched for 21 days. Contact tracing finds new cases quickly, so they can be isolated, stopping further spread of Ebola.
Prevention
Prevention of Ebola HF presents several challenges. The fact that it is still unknown exactly how people are infected with Ebola HF means there are few established primary prevention measures. When infections do occur, there is increased risk of transmission, particularly in healthcare settings. Due to this increased risk, healthcare workers must be able to recognize an infection with Ebola HF and be ready to employ practical viral hemorrhagic fever isolation precautions or barrier nursing techniques. They should also have the ability to request diagnostic testing or to prepare samples for shipping and testing at other locations. Barrier nursing techniques include the following:
- Wearing of protective clothing
- Use of infection control measures
- Isolation of Ebola HF patients from contact with unprotected people
The goal of these techniques is to avoid contact with the secretions or blood of a person who is infected with the virus. If a person with Ebola HF dies, it is just as important that direct contact with the body of the person who has died be prevented.
December 2013 Ebola Outbreak
Experts are calling for a massive global response to tackle Ebola. The outbreak which began in December 2013 now spans five countries in West Africa and has so far killed nearly 2000 people, with the WHO predicting that 20,000 may become infected. (Sept. 2014). In cities like Monrovia in Liberia, the infection has led to the closure of most health facilities, and as a result, untreated injuries and illnesses have caused further loss of life. Exponential growth in numbers makes tracing and surveillance for Ebola increasingly difficult, and that cases could double every fortnight if the situation remains the same.
Professor Piot, Director of the London School of Hygiene & Tropical Medicine, writes:
"This fast pace of Ebola's spread is a grim reminder that epidemics are a global threat and that the only way to get this virus under control is through a rapid response at a massive global scale - much stronger than the current efforts."
This is an opportune time to accelerate evaluation of experimental therapies and vaccines. With the WHO announcing that compassionate use of experimental therapies is ethically justified, even if they have not been tested in humans - An exceptional crisis requires an exceptional response.

New protocol for imaging patients with Ebola:
In a breakthrough that could substantially improve physicians' ability to rapidly evaluate patients with suspected Ebola, radiologists at Emory University Hospital have devised a protocol for obtaining chest radiographs using portable computed radiography. The protocol not only limits the exposure of personnel and equipment to body fluids, it also minimizes the risk of contaminants leaving the isolation unit by use of thorough decontamination procedures. The step-by-step protocol is outlined in an article published ahead of print in the American Journal of Roentgenology.
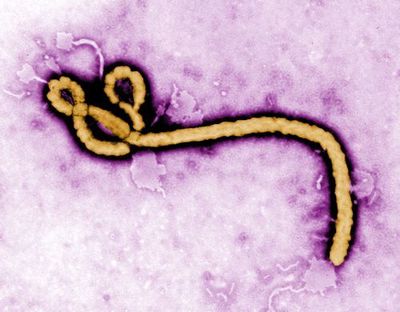
Colorized transmission electron micrograph (TEM) of the Ebola virus. Photo: Frederick A. Murphy, via the Centers for Disease Control and Prevention
Experts question aspects of certain Ebola guidelines (Wiley):
Various guidelines for caring for patients infected with Ebola virus are being issued from different national and state public health authorities, professional societies, and individual hospitals. Experts are questioning aspects of some of the guidelines that go beyond current CDC recommendations, especially those that call for suspending certain routine lab tests.
The authors of a Transfusion commentary note that most individuals with suspected Ebola virus disease will have a fever due to another cause, and forgoing such testing may compromise patients' health more than any reduction in the risks to laboratory personnel.
The authors also state that it is imperative for all laboratory directors to work with institutional infection control and safety personnel to evaluate their hospital policies on potentially infectious patients to provide a safe environment for their patients and employees.
"We are anxious for a balanced, thoughtful discussion of the best way to prepare for the potential of increasing numbers of Ebola suspects across a spectrum of healthcare institutions in the developed world, and believe that the key is recognition of risk and application of well characterized infection prevention and control recommendations," said co-author Dr. Louis Katz. "Suspending aspects of care or automatically transferring patients to other facilities may not be an effective response to the prevention of healthcare-associated transmission if more cases are repatriated than we have seen to date."
Ebola Facts and Statistics
According to the World Health Organization (WHO), Ebola is one of the deadliest viruses known to humankind, and the current outbreak is the largest in history, according to the U.S. Centers for Disease Control and Prevention (CDC).
- From 1976 (when it was first identified) through 2013, the World Health Organization reported 1,716 confirmed cases.
- The average EVD case fatality rate is around 50%. Case fatality rates have varied from 25% to 90% in past outbreaks.
- Ebola has a high risk of death, killing between 25 and 90 percent of those infected, with an average of about 50 percent.
- The largest outbreak to date is the ongoing 2014 West Africa Ebola virus outbreak, which is affecting Guinea, Sierra Leone, Liberia, Mali, and Nigeria. As of 8 March 2015, 24,282 suspected cases and 9,976 deaths had been reported; however, the WHO has said that these numbers may be underestimated.
- The incubation period, that is, the time interval from infection with the virus to onset of symptoms, is 2 to 21 days.
- Humans are not infectious until they develop symptoms.
- First symptoms are the sudden onset of fever fatigue, muscle pain, headache and sore throat.
- This is followed by vomiting, diarrhea, rash, symptoms of impaired kidney and liver function, and in some cases, both internal and external bleeding (e.g., oozing from the gums, blood in the stools).
- Laboratory findings include low white blood cell and platelet counts and elevated liver enzymes.
Ebola Virus Disease Outbreak Updates: Track the evolving Bundibugyo Ebola outbreak in DRC and Uganda: case counts, deaths, cross-border spread, and the latest WHO response and risk levels.
Frequently Asked Questions
Is there a vaccine available to prevent Ebola?
Approved Ebola vaccines now exist for certain virus strains and are used during outbreaks to protect frontline workers and contacts, though availability depends on the specific strain and region involved.
Can you catch Ebola from someone who has no symptoms?
No, people infected with Ebola are not contagious until they begin showing symptoms, which is why isolating symptomatic patients is central to stopping the spread.
How long does it take to recover from Ebola?
Recovery varies by individual, but survivors often need weeks to months to regain strength, and some experience lingering effects such as joint pain, vision problems, and fatigue.
Can Ebola survive on surfaces outside the body?
Ebola can persist for a time on contaminated surfaces and objects, so thorough cleaning, disinfection, and safe disposal of medical instruments are essential during outbreaks.
Is it safe to travel to countries with an active Ebola outbreak?
Travel risk depends on the outbreak's location and scale, and health authorities may issue advisories, so travelers should check current guidance and practice recommended precautions.
Can Ebola be transmitted through the air like the flu?
Ebola does not spread through casual airborne transmission, and instead requires direct contact with infected bodily fluids or contaminated objects to pass between people.
Do Ebola survivors develop immunity to the virus?
Survivors typically develop antibodies that may offer protection against the specific strain they had, though the strength and duration of that immunity is still being studied.
Curated and edited by Ian C. Langtree, Founder & Editor-in-Chief, Disabled World. This section is maintained by the Disabled World editorial team.
Last updated: