Weight Loss Medication Options in 2026
Author: Ian C. Langtree - Writer/Editor for Disabled World (DW)
Published: 20 Apr 2026 - Updated: 3 Aug 2026
Publication Type: Informative
Table of Contents:
Synopsis - Definition - Overview - FAQs - Insights, Updates - Related Content
Synopsis
In less than five years, the pharmacological treatment of obesity has gone from a quiet corner of internal medicine to the most disruptive category in American health care, and the products arriving in 2026 are rewriting what clinicians, courts, and insurers can credibly say about weight, ability, and the machinery of the human body.
At a Glance
- 1 - Alli is the only over-the-counter weight loss drug the FDA has approved.
- 2 - New York City banned weight-based employment discrimination outright in 2023.
- 3 - Zepbound is currently the most effective option on the U.S. market, with about 20 percent mean weight loss.
- 4 - The ADA does not list obesity as a protected condition, though related conditions such as type 2 diabetes, sleep apnea, and severe knee osteoarthritis can each qualify on their own.
Topic Definition
- Weight Loss Medication
A weight loss medication is a prescription or over-the-counter pharmaceutical product approved by a national drug regulator, such as the U.S. Food and Drug Administration, to help adults, and in some cases adolescents, reduce excess body weight and maintain that reduction over time when combined with a reduced-calorie diet and increased physical activity. These medications work through a range of mechanisms, including mimicking gut hormones that regulate appetite and insulin response, suppressing appetite through central nervous system pathways, or blocking the intestinal absorption of dietary fat, and they are delivered as weekly or daily injections, oral tablets, or capsules depending on the specific product.
Overview
Weight Loss Drugs 2026: Brands, Results, Disability
Obesity care in the United States has been rewritten in less than a decade. The pharmacological treatment of obesity used to mean phentermine prescriptions and over-the-counter orlistat at the drugstore, with modest results that often vanished the moment a patient stopped taking the pill. That world still exists, but it now sits alongside a generation of injectable and oral medications that routinely produce double-digit percentage weight loss and are reshaping how physicians, insurers, and courts think about body weight itself (Obesity Medicine Association, 2026).
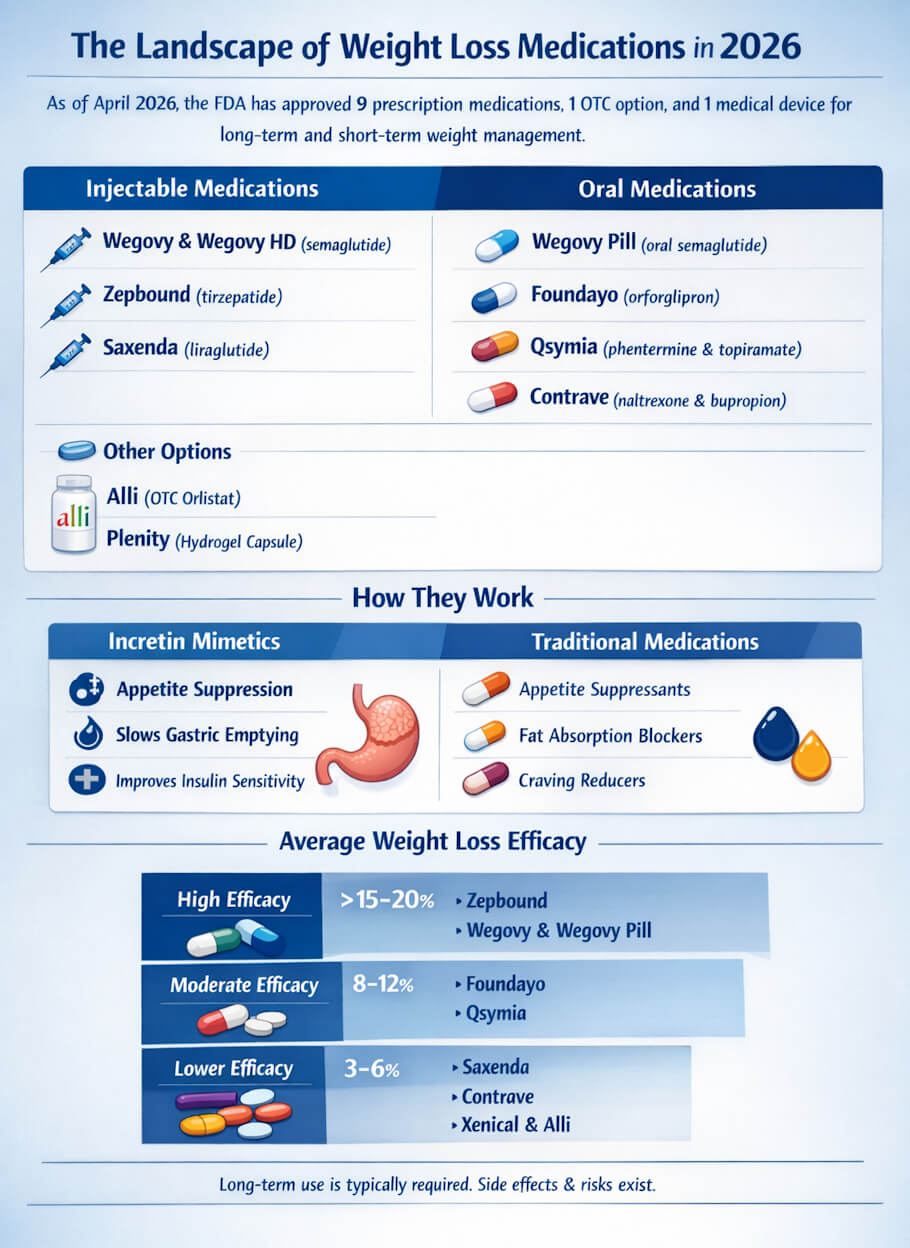
As of April 2026, the U.S. Food and Drug Administration has approved nine pharmacological options for long-term or short-term weight management in adults, along with one medical device classified as a prescription product and a single over-the-counter option. Two of those medications arrived within the last five months: the oral formulation of Wegovy in December 2025 and Foundayo (orforglipron) on April 1, 2026 (U.S. Food and Drug Administration, 2026a). A higher-dose injectable version of Wegovy, branded Wegovy HD, was approved on March 19, 2026 (U.S. Food and Drug Administration, 2026b). The pipeline behind these products is crowded. Analysts at Ozmosi have identified roughly three dozen GLP-1-related weight management candidates in development, with new launches expected every year for the foreseeable future.
How These Medications Actually Work
Most of the newer weight loss drugs belong to a class called incretin mimetics. They imitate hormones the gut releases after meals - glucagon-like peptide-1 (GLP-1) and, in some cases, glucose-dependent insulinotropic polypeptide (GIP). These hormones slow gastric emptying, blunt appetite signals in the brain, and improve insulin sensitivity. The older medications work differently: some are stimulants that suppress appetite (phentermine), some block fat absorption in the intestine (orlistat), and some combine neuromodulators that reduce reward-driven eating (Contrave).
The practical distinction that matters most to patients is simpler than the pharmacology. Some of these products are injected under the skin, usually once a week. Others are swallowed. Some require a prescription and physician supervision. Only one true anti-obesity drug is sold without a prescription in the United States.
Injectable Prescription Medications
Wegovy (semaglutide)
Manufactured by Novo Nordisk and approved in 2021 for chronic weight management, Wegovy delivers semaglutide once weekly by subcutaneous injection using a pre-filled pen. Phase 3 trials reported mean weight reduction of roughly 14.9% of body weight over 68 weeks at the 2.4 mg dose. The drug is approved for adults with a body mass index (BMI) of 30 or higher, or 27 or higher with at least one weight-related comorbid condition, and for adolescents 12 and older with a BMI at or above the 95th percentile. In March 2026 the FDA approved a higher 7.2 mg dose called Wegovy HD, which produced additional weight reduction beyond the standard dose in clinical testing (U.S. Food and Drug Administration, 2026b).
Zepbound (tirzepatide)
Eli Lilly's Zepbound, approved for obesity in late 2023, is currently the most effective weight loss medication on the U.S. market. It is a dual GLP-1 and GIP receptor agonist administered once weekly by injection. In the head-to-head SURMOUNT-5 trial published in The New England Journal of Medicine, tirzepatide produced a mean weight reduction of 20.2% at 72 weeks compared with 13.7% for semaglutide, the first direct clinical comparison of the two (Aronne et al., 2025). A separate phase 3 trial in participants with knee osteoarthritis and obesity found weight losses of up to 28.7% with the related triple-agonist retatrutide, which remains in development but signals where this class is heading.
Saxenda (liraglutide)
Liraglutide, marketed by Novo Nordisk as Saxenda, was the first GLP-1 receptor agonist approved for weight management in adults and is also approved for adolescents 12 and older. Unlike Wegovy and Zepbound, it must be injected daily rather than weekly. Its weight loss effect is more modest, typically 5% to 8% of body weight at 56 weeks, but it remains relevant for patients who cannot tolerate the newer agents or whose insurance favors it on formulary.
Oral Prescription Medications
Wegovy Pill (oral semaglutide for obesity)
In December 2025 the FDA approved an oral formulation of Wegovy, the first oral GLP-1 receptor agonist cleared specifically for chronic weight management. At the highest dose, trial participants lost an average of 16.6% of their body weight after 64 weeks, and roughly one in three lost at least 20% (AARP, 2026). The pill is taken once daily on an empty stomach with a small amount of water, a protocol some patients find inconvenient. A lower-dose oral semaglutide product called Rybelsus has been available since 2019 for type 2 diabetes and is sometimes prescribed off label.
Foundayo (orforglipron)
Approved on April 1, 2026, Foundayo is Eli Lilly's oral GLP-1 receptor partial agonist and the only weight loss pill of its class that can be taken any time of day without food or water restrictions. Its chemistry - a small-molecule nonpeptide rather than a peptide - makes it more stable in the stomach. In the ATTAIN-1 trial, adults taking the highest dose of 36 mg lost an average of 12.4% of body weight, about 27 pounds, after 72 weeks, compared with about 2 pounds for placebo (Eli Lilly and Company, 2026). Foundayo was the first new molecular entity approved under the FDA's Commissioner's National Priority Voucher program, which shortened the review timeline by several months (U.S. Food and Drug Administration, 2026a).
Qsymia (phentermine and topiramate)
Qsymia combines a controlled-substance appetite suppressant (phentermine) with the anticonvulsant topiramate in an extended-release capsule. It is approved for chronic weight management in adults and in pediatric patients 12 and older. Mean weight loss in trials runs about 8% to 10% at one year. It requires prescriber enrollment in a Risk Evaluation and Mitigation Strategy because of the teratogenic potential of topiramate.
Contrave (naltrexone and bupropion)
Contrave pairs a low-dose opioid antagonist with an antidepressant to reduce appetite and cravings. It produces roughly 5% to 6% mean weight loss at one year. The combination can raise blood pressure and is contraindicated in patients taking opioids, so clinician selection matters.
Phentermine (Adipex-P, Lomaira)
Phentermine is the oldest and cheapest prescription weight loss medication still in wide use, originally approved in 1959. It is a sympathomimetic amine sold as Adipex-P, Lomaira, and under its generic name. It is FDA approved only for short-term use, generally up to 12 weeks, because of its stimulant profile and potential for tolerance. Many clinicians prescribe it in cycles or alongside topiramate. It remains popular in part because generic monthly costs can fall below $15 without insurance.
Xenical (prescription orlistat)
Orlistat, marketed at the 120 mg prescription strength as Xenical, inhibits pancreatic lipase and blocks absorption of about 30% of dietary fat. Average weight loss is 3% to 5% at one year. Its gastrointestinal side effects - oily stools, flatulence, fecal urgency when patients eat high-fat meals - are well known and are the reason many patients discontinue it.
Over-the-Counter and Device-Based Options
Alli (orlistat 60 mg)
Alli is the only over-the-counter weight loss medication approved by the FDA. It contains orlistat at half the prescription strength and is available on drugstore shelves for adults 18 and older with a BMI of 25 or higher. Its efficacy and side effect profile mirror those of Xenical at a smaller magnitude. Alli remains useful for patients who want a nonprescription option and are willing to maintain a low-fat diet during treatment.
Plenity (prescription, not an OTC drug)
Plenity is often mentioned alongside medications but is technically a prescription medical device rather than a drug. It is a hydrogel made of carboxymethylcellulose and citric acid that expands in the stomach to create a feeling of fullness. Patients take three capsules with water before lunch and dinner. Mean weight loss in the gateway trial was about 6.4%. Because it is classified as a device, it is regulated and reimbursed differently than the GLP-1 products.
How the Medications Compare for Efficacy
Ranked roughly by average percent body weight loss at one year or longer, the current options fall into three tiers. At the top sit Zepbound at about 20% mean loss, followed by injectable Wegovy at about 15% and the Wegovy pill at about 17% at the highest dose (Aronne et al., 2025; AARP, 2026). Foundayo sits near the middle at 12.4%, a meaningful but smaller effect than the injectables (Eli Lilly and Company, 2026). Qsymia, Saxenda, and Plenity land in the 5% to 10% range. Contrave, Xenical, and Alli typically produce 3% to 6%.
These numbers are averages. Individual response varies widely. Roughly one in five patients on GLP-1 drugs is a low responder, and up to a third lose more than 20% of their starting weight. Weight regain after discontinuation is common and often substantial, which is why most clinicians frame these medications as chronic therapies for a chronic disease rather than short courses.
The Overlap Between Weight Loss and Disability
Weight enters disability law through several doors, and none of them are wide. The Americans with Disabilities Act (ADA) does not list obesity as a protected condition, and federal courts have been reluctant to treat body weight alone as a qualifying disability.
Obesity Under the Americans with Disabilities Act
The ADA defines disability as a physical or mental impairment that substantially limits one or more major life activities. The implementing regulations of the Equal Employment Opportunity Commission specifically exclude physical characteristics within a normal range, including weight, unless they result from a physiological disorder. Four federal circuit courts - the Second, Sixth, Seventh, and Eighth - have held that obesity is not an ADA impairment unless it is caused by an underlying physiological condition (Richardson v. Chicago Transit Authority, 2019). The most cited case, Richardson, involved a Chicago bus driver whose weight rose above 550 pounds; the court declined to recognize his obesity as a disability because he produced no evidence of a physiological cause.
State and municipal law fills some of the gap. New York City banned weight-based employment discrimination outright in 2023. Michigan and a handful of cities including San Francisco, Washington D.C., and Binghamton maintain similar protections. Courts in Texas, Louisiana, Mississippi, California, New Jersey, New York state, Washington, and Oregon have been more willing than their federal counterparts to recognize obesity, or perceived obesity, as a qualifying condition in disability discrimination claims (Ogletree, 2023).
Weight-Related Comorbidities That Do Qualify
Where weight itself falls outside the ADA, the conditions that commonly accompany it often do not. Type 2 diabetes, obstructive sleep apnea, severe osteoarthritis of the knees or hips, congestive heart failure, lymphedema, and chronic kidney disease can each independently meet the ADA definition of disability when they substantially limit a major life activity. A warehouse worker with knee osteoarthritis severe enough to limit standing or walking is protected under the statute regardless of the number on the scale. This distinction is legally important and, in practice, is how many large employees pursue accommodation rather than arguing obesity on its own terms.
How Weight Loss Medication Can Change the Disability Picture
The new generation of GLP-1 medications is starting to alter the clinical calculus around weight-related disability. Beyond weight reduction, semaglutide has demonstrated improved cardiovascular outcomes and reduced progression of diabetic kidney disease, and tirzepatide has been shown to reduce liver fat, improve metabolic dysfunction-associated steatohepatitis, and decrease the severity of obstructive sleep apnea (American Diabetes Association, 2024). The TRIUMPH-4 trial of retatrutide reported substantial reduction in knee osteoarthritis pain alongside weight loss. As these indications expand, more patients may find that the underlying impairments limiting their work lives - joint pain, apnea-driven fatigue, uncontrolled diabetes - respond to a weekly injection. That does not make the medications a substitute for reasonable accommodation. It does mean the clinical picture of a disabled worker with obesity is less static than it was five years ago.
Access, Insurance, and the Practical Barriers
Coverage is the quiet crisis underneath the excitement about these drugs. List prices for Wegovy and Zepbound run roughly $1,000 to $1,350 per month before rebates. Medicare Part D historically excluded weight loss drugs by statute, though that has begun to shift for obesity-related conditions such as cardiovascular disease. Commercial coverage is uneven. Manufacturer self-pay programs have narrowed the gap: Foundayo launched at $149 per month for its lowest dose on self-pay and $25 per month with the manufacturer savings card for those with commercial insurance (Eli Lilly and Company, 2026). A FAIR Health analysis published in May 2025 reported that more than 2% of U.S. adults had filled a prescription for a GLP-1 weight loss medication in the preceding year, a share that has since grown.
For patients who qualify as disabled under state law or the ADA through an underlying condition, the calculus shifts again. Some state Medicaid programs now cover anti-obesity medications when a comorbid disability is documented, and several federal accommodations claims have successfully argued that denial of effective weight management treatment constitutes a failure to accommodate a physiological condition.
Risks and Realistic Expectations
None of these medications is benign. Gastrointestinal side effects - nausea, vomiting, constipation, diarrhea - are the most common reason patients discontinue GLP-1 drugs. Rarer but serious risks include pancreatitis, gallbladder disease, and a boxed warning for thyroid C-cell tumors observed in rodent studies. Orlistat can cause liver injury in rare cases and interferes with absorption of fat-soluble vitamins. Phentermine carries the cardiovascular risks typical of stimulants. Qsymia requires pregnancy prevention counseling due to topiramate. Contrave is contraindicated in patients with seizure disorders or eating disorders.
Muscle loss during rapid weight reduction is a concern specific to the GLP-1 class. Clinicians now routinely recommend resistance training and a minimum of 30 grams of protein per meal during active treatment (American Diabetes Association, 2024). The combination of an amylin analog, cagrilintide, with semaglutide - known as CagriSema - is in late-stage development and has reported mean weight loss of 20.4% at 68 weeks with less muscle loss than semaglutide alone in early results (Obesity Medicine Association, 2026).
Weight loss medication works best when patients, physicians, and payers treat obesity as what the American Medical Association has called it since 2013: a chronic disease. That framing has not yet fully reached the courts, and it has only partly reached the insurance market. But it is the clinical reality the next decade of these products will be built on.
References:
AARP. (2026, April 2). FDA approves new weight loss pills: Costs and results. AARP Health.
American Diabetes Association. (2024). Starting FDA-approved weight management medications. Professional Resources.
Aronne, L. J., Horn, D. B., le Roux, C. W., Ho, W., Falcon, B. L., Gomez Valderas, E., Das, S., Lee, C. J., Glass, L. C., Senyucel, C., and Dunn, J. P. (2025). Tirzepatide as compared with semaglutide for the treatment of obesity. The New England Journal of Medicine, 393(16), 1543 - 1554.
Eli Lilly and Company. (2026, April 1). FDA approves Lilly's Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions [Press release]. PR Newswire.
Ghusn, W., De La Rosa, A., Sacoto, D., Cifuentes, L., Campos, A., Feris, F., Hurtado, M. D., and Acosta, A. (2022). Weight loss outcomes associated with semaglutide treatment for patients with overweight or obesity. JAMA Network Open, 5(9), e2231982.
Obesity Medicine Association. (2026, April 2). Top weight loss medications. OMA Clinical Resources.
Ogletree Deakins. (2023). Obesity as a disability under the Americans with Disabilities Act. Employment Law Insights.
Richardson v. Chicago Transit Authority, 926 F.3d 881 (7th Cir. 2019).
U.S. Equal Employment Opportunity Commission. (2008). Enforcement guidance on the Americans with Disabilities Act and the ADA Amendments Act. Washington, DC: EEOC.
U.S. Food and Drug Administration. (2026a, April 1). FDA approves first new molecular entity under National Priority Voucher program [Press release].
U.S. Food and Drug Administration. (2026b, March 19). FDA approves fourth product under National Priority Voucher program, higher dose semaglutide [Press release].
University of Chicago Law Review. (2024). Weighing in: Why obesity should be considered a qualifying disability under the Americans with Disabilities Act. The University of Chicago Law Review, 91(3), 789 - 828.
Frequently Asked Questions
Are GLP-1 weight loss medications safe to use during pregnancy
GLP-1 medications are generally not recommended during pregnancy, and some combination products such as Qsymia require pregnancy prevention counseling because of birth defect risk, so anyone who is pregnant or planning to conceive should speak with a clinician.
Can you take weight loss medication and diabetes medication together
Many of these drugs began as diabetes treatments, so combined use is common but must be supervised by a prescriber to manage blood sugar and avoid overlapping mechanisms.
How long does a person usually stay on weight loss medication
Because obesity is treated as a chronic condition and weight often returns after stopping, most clinicians frame these drugs as long-term therapy rather than a short course.
Do weight loss medications require a change in diet and exercise
Yes, they are approved for use alongside a reduced-calorie diet and increased physical activity, and results are generally better when those habits are maintained.
What can a patient do if a GLP-1 drug is not covered by insurance
Options include manufacturer self-pay programs and savings cards, checking whether a documented comorbid condition unlocks coverage, and discussing lower-cost older medications with a clinician.
Is there an age limit for starting weight loss medication
Several products are approved only for adults, while a few, such as Wegovy, Saxenda, and Qsymia, are also cleared for adolescents aged 12 and older under medical supervision.
How can patients protect muscle while losing weight on these drugs
Clinicians commonly recommend resistance training and adequate protein, often at least 30 grams per meal, to reduce muscle loss during rapid weight reduction.
Insights, Analysis, and Developments
Editorial Note: None of these medications is a finished answer to obesity, and none resolves the uncomfortable questions about who gets access, what insurance will pay for, and where the law draws the line between a body and a disability - but the next several years will force every one of those questions into the open, whether the system is ready or not.
 Author Credentials: Ian is the founder and Editor-in-Chief of Disabled World, a leading resource for news and information on disability issues. With a global perspective shaped by years of travel and lived experience, Ian is a committed proponent of the Social Model of Disability-a transformative framework developed by disabled activists in the 1970s that emphasizes dismantling societal barriers rather than focusing solely on individual impairments. His work reflects a deep commitment to disability rights, accessibility, and social inclusion. To learn more about Ian's background, expertise, and accomplishments, visit his full biography.
Author Credentials: Ian is the founder and Editor-in-Chief of Disabled World, a leading resource for news and information on disability issues. With a global perspective shaped by years of travel and lived experience, Ian is a committed proponent of the Social Model of Disability-a transformative framework developed by disabled activists in the 1970s that emphasizes dismantling societal barriers rather than focusing solely on individual impairments. His work reflects a deep commitment to disability rights, accessibility, and social inclusion. To learn more about Ian's background, expertise, and accomplishments, visit his full biography.