Bundibugyo Ebola Outbreak Updates: DR Congo and Uganda (2026)
Author: Ian C. Langtree - Writer/Editor for Disabled World (DW)
Published: 9 Jun 2026 - Updated: 17 Jul 2026
Publication Type: Informative
Table of Contents:
Synopsis - Definition - Overview - Insights, Updates - Related Content
Synopsis
This report follows the 2026 outbreak of Bundibugyo virus disease, a species of Ebola, as it spreads through the Democratic Republic of the Congo and Uganda, gathering dated entries begin mid-May against official figures published in World Health Organization Disease Outbreak News. Its value lies in resting on primary public health reporting and updating as conditions change, logging confirmed cases, deaths, case fatality rates, affected health zones, and cross-border transmission..At a Glance
- 1 - Health workers account for a significant share of cases and deaths, revealing gaps in infection prevention and control practices.
- 2 - A French doctor who had treated patients in Ituri tested positive after returning home, prompting isolation and contact tracing in both France and DRC.
- 3 - The response is complicated by a conflict-affected environment marked by displacement, crowded camps, limited access to clean water and healthcare, and security incidents disrupting operations.
Topic Definition
- Ebola Virus Disease
Ebola virus disease (EVD), also known as Ebola hemorrhagic fever or simply Ebola, is a severe and often fatal illness affecting humans and other primates, caused by viruses of the family Filoviridae, genus Ebolavirus. The virus passes to people from wild animals and then spreads through human-to-human transmission, typically by direct contact with the blood or secretions of an infected person or with contaminated objects such as needles. After an incubation period of two days to three weeks, it generally begins with fever, sore throat, muscle pain, and headache, followed by vomiting, diarrhea, rash, reduced liver and kidney function, and in some cases internal and external bleeding. Of the five identified subspecies, four have caused disease in people, making Ebola one of the deadliest viruses known to humankind.
Overview
Suspected Cause
Bundibugyo virus is a zoonotic Orthoebolavirus species, with fruit bats suspected as the natural reservoir, that spreads person-to-person through contact with bodily fluids and is amplified in healthcare settings and during unsafe burials. Its two-to-21-day incubation period and non-specific early symptoms make it hard to distinguish from illnesses like malaria without lab confirmation, and there are currently no approved vaccines or specific treatments, so control depends on rapid detection, isolation, contact tracing, and community engagement.
Risk to the U.S.
On May 18, CDC and DHS announced enhanced travel screening, entry restrictions, and public health measures to prevent Ebola disease from entering the United States amid outbreaks in East and Central Africa. To date, no Ebola cases associated with this outbreak have been reported in the United States, and the risk to the general public remains low.
Symptoms of Ebola Image

Ebola Outbreak Updates - 2026
17th July, 2026
This WHO Disease Outbreak News update describes a still-active and worsening outbreak of Ebola disease caused by Bundibugyo virus (BVD), centered in the Democratic Republic of the Congo with continued links to Uganda, France, and Germany. As of July 15, the DRC had recorded 2,124 confirmed cases and 828 deaths, a crude case fatality ratio of roughly 39 percent, spread across 46 health zones in five provinces (Ituri, North Kivu, South Kivu, Haut-Uele, and Tshopo), with Ituri bearing nearly 90 percent of cases and about 84 percent of deaths. Uganda reported no new cases since June 21, holding at 20 confirmed cases and two deaths among imported cases, and discharged its most recent patient on July 16, beginning the 42-day countdown before the outbreak there can be declared over. Across all locations, 2,145 confirmed cases and 830 deaths have been tallied, with at least 410 patients recovered. Germany also reported a second U.S. citizen, a humanitarian worker medically evacuated from the DRC in July, now in stable condition.
The report notes that the sharp rise in the DRC, an additional 664 confirmed cases and 376 deaths since July 3, stems partly from scaled-up surveillance, testing, and diagnostics, with the outbreak remaining active in 38 of 46 affected health zones and heavy clusters in Bunia, Rwampara, and Mongbwalu. Health workers continue to be hard hit, with 119 confirmed cases and 36 deaths (a 30.3 percent fatality ratio), reflecting persistent gaps in infection prevention and control. More than 12,600 contacts are under follow-up across affected provinces, with completion rates ranging from about 50 to 92 percent. The response remains hampered by a conflict-affected, humanitarian setting marked by displacement, crowded camps, limited access to clean water and healthcare, and security incidents disrupting operations. In France, the single imported case recovered and was discharged, with all flight contacts completing follow-up and no secondary transmission detected.
Finally, WHO's risk assessment rates the situation as very high within the DRC due to ongoing transmission and expansion into new health zones, high in Uganda and in neighboring countries sharing land borders with affected areas, and low for the rest of the African region and globally. WHO continues to advise against any travel or trade restrictions to the DRC or Uganda based on current information, while emphasizing coordinated cross-border surveillance and preparedness under the temporary recommendations issued in May 2026. The agency reiterates that no approved vaccines or specific treatments currently exist for BVD, that control depends on rapid detection, isolation, contact tracing, safe burials, and community engagement, and that expert groups including the Strategic Advisory Group of Experts on Immunization continue to evaluate candidate vaccines and therapeutics as regular epidemiological reports track the outbreak's evolution.
Full report from WHO: who.int/emergencies/emergency-events/item/2026-e000253
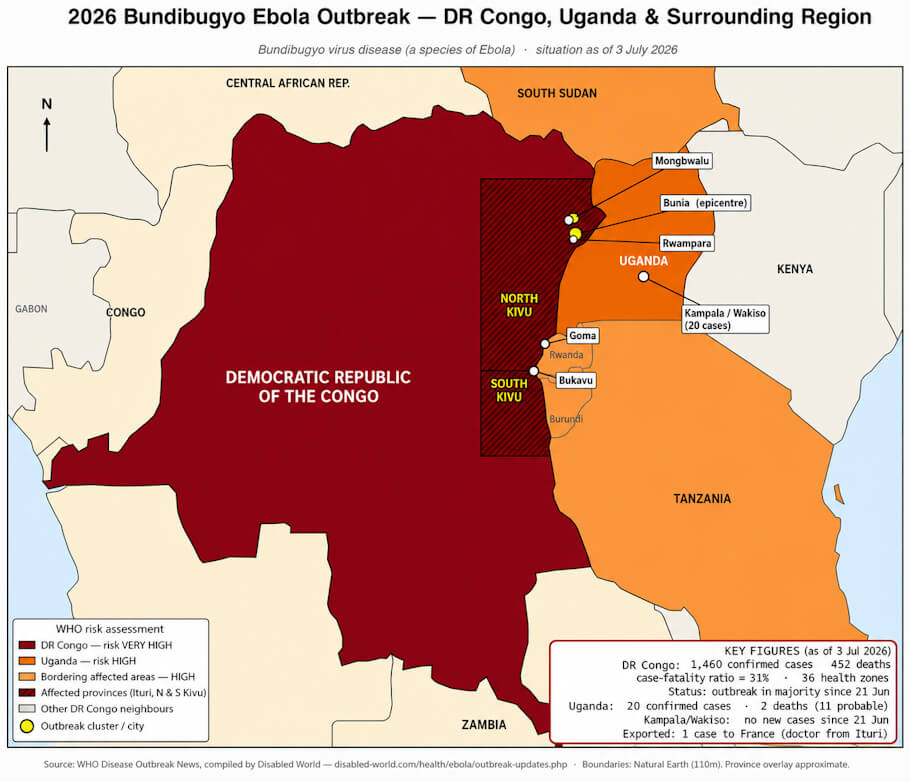
3rd July, 2026
This WHO Disease Outbreak News update (dated July 3, 2026) describes an escalating outbreak of Ebola disease caused by Bundibugyo virus (BVD) centered in the Democratic Republic of the Congo, with spillover into Uganda and one exported case to France. As of July 1, DRC had recorded 1,460 confirmed cases and 452 deaths (a case fatality ratio near 31%), spread across 36 health zones in Ituri, North Kivu, and South Kivu provinces, with Ituri bearing the overwhelming majority of the burden. Uganda, as of July 2, had reported 20 confirmed cases (two deaths) plus one fatal probable case, all linked epidemiologically to the DRC outbreak, with no new cases since June 21 and no confirmed community transmission. A French medical doctor who had been treating BVD patients in Ituri also tested positive after returning home, prompting isolation and contact tracing in both France and DRC.
The report details how the outbreak's growth in DRC is being driven partly by expanded surveillance and testing, with transmission continuing in 21 of the 36 affected health zones and notable clusters in Bunia, Rwampara, and Mongbwalu. Health workers account for over a hundred cases and multiple deaths, underscoring gaps in infection prevention and control. The response is complicated by a humanitarian and conflict-affected environment marked by displacement, crowded camps, limited access to clean water and healthcare, and security incidents disrupting response operations. Thousands of contacts are under monitoring in both DRC and Uganda, with follow-up completion rates above 80%. The page also explains BVD's epidemiology as a zoonotic, bat-borne Orthoebolavirus with a two-to-21-day incubation period, nonspecific early symptoms, and historical case fatality rates of 30-50% in past outbreaks, noting there are still no approved vaccines or specific treatments.
Finally, WHO's risk assessment rates the situation as very high within DRC, high in Uganda and in neighboring countries sharing land borders with the affected areas, and low for the rest of the African region and globally. WHO advises against any travel or trade restrictions to DRC or Uganda based on current information, while emphasizing coordinated cross-border surveillance and preparedness under temporary recommendations issued in May 2026. The agency has also convened expert groups, including the Strategic Advisory Group of Experts on Immunization, to evaluate candidate vaccines and therapeutics, and continues to publish regular epidemiological updates, situation reports, and outbreak news bulletins tracking the event's evolution.
19th June, 2026
The Bundibugyo virus disease (BVD) outbreak centered in the Democratic Republic of the Congo is escalating rapidly. As of 17 June 2026, the DRC has recorded 896 confirmed cases and 232 deaths (a case fatality ratio of about 26%, likely an underestimate), with 220 of those cases and 96 deaths added since the prior report on 13 June-partly because expanded testing cleared a backlog of older samples. The outbreak spans 33 health zones across Ituri, North Kivu, and South Kivu, but remains heavily concentrated in Ituri Province, which accounts for roughly 91% of confirmed cases, with Bunia, Rwampara, and Mongbwalu the hardest-hit zones. Some newly reporting areas likely reflect previously undetected transmission that had been ongoing for weeks rather than fresh spread.
In Uganda, the situation is far more contained and linked epidemiologically to the DRC outbreak. As of 18 June, Uganda had 19 confirmed cases (14 imported, 5 from secondary transmission among contacts and health workers) plus one probable case, with two confirmed deaths and one probable death. Cases are confined to Kampala and Wakiso districts within the Kampala Metropolitan Area, with no documented community transmission and exposure tied to healthcare settings and cross-border movement. Notably, Uganda has reported no new cases since 5 June 2026. Across both countries, 88 patients have recovered (78 in the DRC, 10 in Uganda), and extensive contact tracing is underway-6,367 contacts followed in the DRC and 826 listed in Uganda.
The response is complicated by the operating environment in eastern DRC, where conflict, insecurity, and large displaced and highly mobile populations strain access to food, clean water, shelter, and healthcare. Security incidents affecting health facilities have disrupted surveillance and response activities and raised the risk of undetected transmission, underscoring the need for community- and locally-led efforts. National authorities in both countries, working with WHO and partners, are implementing a broad set of response measures, guided by a regional preparedness and prioritization framework across the African Region.
13th June, 2026
By mid-June the Bundibugyo virus disease outbreak had grown to 695 confirmed cases and 138 deaths across the two countries. DR Congo carried almost the entire burden, with 676 confirmed cases and 136 deaths, a case fatality rate near 20 percent, while at least 37 people had recovered. The DRC caseload now stretches across 29 health zones in Ituri, North Kivu, and South Kivu, with Ituri remaining the epicenter and accounting for the overwhelming majority of infections. Uganda's tally held at 19 confirmed cases, two confirmed deaths, and one probable death, all traceable to the DRC through imported infections and a small number of secondary cases among contacts and health workers; notably, the country had logged no new cases in about six days and still had no sign of community transmission.
In clinical terms, Bundibugyo virus is a zoonotic Ebola species linked to fruit bats as its likely reservoir, passing between people through contact with infected bodily fluids and spreading fastest where infection control is weak or where burials bring mourners into direct contact with the deceased. Its incubation window of two to 21 days and its vague early symptoms, fever, fatigue, aching muscles, headache, and sore throat, make it easy to mistake for malaria or other common fevers until the illness advances toward organ failure and bleeding. With no licensed vaccine or specific cure available, containment still rests on finding cases quickly, isolating patients, tracing contacts, conducting safe burials, and keeping affected communities engaged, all of which is harder in a region marked by displacement, conflict, and attacks on health facilities.
On the response side, the two governments, WHO, and partner agencies are running a coordinated effort that pairs field operations with fundraising to close persistent gaps. A subnational risk analysis has flagged 159 DRC health zones as affected or at risk, signaling the scale of the work ahead, and authorities are preparing a clinical trial of candidate therapeutics, MBP134 and REGN3479 for treatment and obeldesivir for post-exposure prophylaxis, pending ethical and regulatory sign-off. WHO rates the threat as very high inside the DRC, high in Uganda and in countries sharing land borders with the affected nations, and low for the rest of Africa and the wider world, while continuing to advise against any travel or trade restrictions on either country.
8th June, 2026
The WHO Disease Outbreak News page reports on a rapidly escalating outbreak of Bundibugyo virus disease, a severe form of Ebola, spreading across the Democratic Republic of the Congo and Uganda. As of 6 June 2026, the two countries had reported a combined 534 confirmed cases and 93 deaths, giving a case fatality rate of around 17%, with at least 17 people recovered. Case numbers have climbed sharply since the previous update on 29 May, driven partly by expanded testing that cleared a backlog of previously collected samples.
The bulk of the outbreak is in the DRC, which accounts for 515 confirmed cases and 91 deaths across 25 health zones in Ituri, North Kivu, and South Kivu provinces. Ituri Province is the epicenter, holding the vast majority of cases, though North Kivu shows a far higher fatality rate. Uganda has reported 19 confirmed cases and several deaths, all epidemiologically linked to travelers from the DRC, with no documented community transmission. One notable case involved a Congolese national who traveled through Uganda to the United Arab Emirates and back, prompting cross-border contact tracing, though no secondary spread was identified in the UAE. Security incidents affecting health facilities in the DRC are complicating surveillance and response efforts.
On the response side, authorities in both countries, working with WHO and partners, are coordinating field teams, strengthening surveillance and laboratory capacity, and setting up treatment centers. On 5 June, Africa CDC and WHO launched a joint continental preparedness and response plan seeking US$518 million. WHO assesses the risk as very high in the DRC, high in Uganda and neighboring border countries, and low for the rest of Africa and globally, while advising against any travel or trade restrictions on the affected countries.
29th May, 2026
The BVD outbreak in the Democratic Republic of the Congo and Uganda continued to evolve rapidly, with rising case numbers, wider geographic spread, and ongoing cross-border transmission. As of 27 May, the DRC had reported 906 suspected cases and 223 deaths among suspected cases. As of 29 May, a total of 134 confirmed cases - including nine in Uganda - and 18 deaths among confirmed cases had been reported across both countries, giving a case fatality rate of about 14 percent. This represented an additional 49 confirmed cases, eight confirmed deaths, 160 suspected cases, and 47 suspected deaths since the 21 May update. Separately, a medical doctor from the United States, who had been exposed while caring for patients in the DRC, tested positive on 17 May and was transported to Germany for treatment and care.
In the DRC, transmission remained concentrated in Ituri Province, which accounted for 88 percent of confirmed cases, along with North Kivu and South Kivu provinces. The highest case numbers in Ituri were reported from the Bunia, Rwampara, Mongbwalu, and Nyankunde Health Zones, and 16 confirmed cases had been reported among health and care workers. Security incidents against health facilities and community resistance emerged as major operational challenges, with recent incidents in the Mongbwalu and Rwampara Health Zones creating additional risks of undetected transmission. In Uganda, the nine confirmed cases were reported in Kampala and Wakiso, with exposure risks linked to health-care settings and cross-border movement.
On 22 May 2026, WHO assessed the risk of the outbreak as very high at the national level in the DRC, high at the regional level, and low at the global level. WHO Director-General Dr Tedros Adhanom Ghebreyesus traveled to the DRC on 28 May to support the response. WHO advised against any restriction of travel to, or trade with, the DRC or Uganda based on the information available. National authorities, working with WHO and partners, continued to deploy rapid response teams, deliver medical supplies, strengthen surveillance and laboratory confirmation, reinforce infection prevention and control, establish safe and optimized treatment centers, and prioritize community engagement.
21st May, 2026
Following the declarations of 15 May 2026, when the DRC Ministry of Public Health, Hygiene and Social Welfare and the Uganda Ministry of Health declared an Ebola Disease outbreak after BVD was confirmed in both countries, and the 17 May 2026 PHEIC determination by the WHO Director-General, the response continued to expand. On 19 May 2026, the Director-General convened the first meeting of the IHR Emergency Committee, and temporary recommendations were issued to States Parties.
As of 21 May, the DRC had reported 746 suspected cases and 176 deaths among those suspected cases. Across both countries, 85 confirmed cases - including two in Uganda - and 10 deaths among confirmed cases, one of them in Uganda, had been reported. In the DRC, transmission was concentrated in Ituri, North Kivu, and South Kivu provinces, with challenges in contact follow-up, insecure conditions, and inadequate isolation and referral systems complicating response efforts. Uganda reported two imported cases with no confirmed local transmission. An American national who had been working in the DRC was also confirmed positive and transferred to Germany for care.
National authorities, in collaboration with WHO and partners, continued to implement response measures including the deployment of rapid response teams, delivery of medical supplies, strengthened surveillance, laboratory confirmation, infection prevention and control assessments, the set-up of safe and optimized treatment centers, and community engagement.
16th May, 2026
On 5 May 2026, the World Health Organization (WHO) was alerted to a high-mortality outbreak of an unknown illness in the Mongbwalu Health Zone, Ituri Province, in the Democratic Republic of the Congo (DRC), including deaths among health workers. On 14 May 2026, the Institut national de recherche biomédicale (INRB) in Kinshasa analyzed 13 blood samples drawn from the Rwampara Health Zone in Ituri Province. The following day, 15 May, laboratory analysis confirmed Bundibugyo virus disease (BVD), a species of Ebola, in eight of those samples.
Case fatality rates in the past two BVD outbreaks have ranged from 30 percent to 50 percent. Unlike Ebola virus disease, there is no licensed vaccine or specific therapeutic against Bundibugyo virus, although early supportive care can be lifesaving. On 15 May 2026, the Ministry of Public Health, Hygiene and Social Welfare in the DRC officially declared the country's 17th Ebola Disease outbreak. At the same time, the Uganda Ministry of Health confirmed an outbreak of BVD after identifying one imported case from the DRC - a Congolese man who died in the capital city of Kampala.
On 17 May 2026, after consulting the States Parties where the event was known to be occurring, the WHO Director-General determined that the Ebola disease caused by Bundibugyo virus in the DRC and Uganda constituted a public health emergency of international concern (PHEIC), as defined under the International Health Regulations (IHR). Response measures at this stage included the deployment of rapid response teams, delivery of medical supplies, strengthened surveillance, laboratory confirmation, infection prevention and control assessments, the establishment of safe treatment centers, and community engagement. WHO supported the coordination of the response, case management, and cross-border preparedness, and issued advice to countries.
Insights, Analysis, and Developments
Editorial Note: Read as a timeline rather than a single bulletin, this page is most useful when revisited, since each dated entry preserves what was known at that point and the totals move quickly as testing widens and backlogged samples are confirmed. Following it over days or weeks shows not only how case counts and fatality rates shifted, but how the response took shape, from the first laboratory confirmation and the public health emergency declaration through cross-border contact tracing and the groundwork for candidate therapeutics under trial conditions. Author Credentials: Ian is the founder and Editor-in-Chief of Disabled World, a leading resource for news and information on disability issues. With a global perspective shaped by years of travel and lived experience, Ian is a committed proponent of the Social Model of Disability-a transformative framework developed by disabled activists in the 1970s that emphasizes dismantling societal barriers rather than focusing solely on individual impairments. His work reflects a deep commitment to disability rights, accessibility, and social inclusion. To learn more about Ian's background, expertise, and accomplishments, visit his full biography.
Author Credentials: Ian is the founder and Editor-in-Chief of Disabled World, a leading resource for news and information on disability issues. With a global perspective shaped by years of travel and lived experience, Ian is a committed proponent of the Social Model of Disability-a transformative framework developed by disabled activists in the 1970s that emphasizes dismantling societal barriers rather than focusing solely on individual impairments. His work reflects a deep commitment to disability rights, accessibility, and social inclusion. To learn more about Ian's background, expertise, and accomplishments, visit his full biography.