Orthostatic Intolerance: Symptoms, Causes, Disability
Author: Ian C. Langtree - Writer/Editor for Disabled World (DW)
Published: 8 May 2026 - Updated: 7 Jun 2026
Publication Type: Informative
Table of Contents:
Synopsis - Definition - Overview - Insights, Updates - Related Content
Synopsis
This article examines orthostatic intolerance (OI), a group of cardiovascular and autonomic conditions in which standing upright triggers symptoms that ease with sitting or lying down, exploring the physiology behind the disorder, the most common forms it takes, the practical ways it limits daily life, and the legal pathways through which OI is recognized as a disability under the Americans with Disabilities Act and the Social Security system.
At a Glance
- 1 - When a person stands up, gravity pulls roughly 500 to 1,000 milliliters of blood downward into the abdomen and lower limbs, and a healthy body must rapidly compensate within seconds to keep blood flowing to the brain.
- 2 - POTS affects young adults with women outnumbering men by roughly four or five to one, and it has drawn increased attention because of its overlap with Long COVID and ME/CFS.
- 3 - Vasovagal syncope is the most common cause of fainting in the general population, with a lifetime prevalence approaching 22 percent.
Topic Definition
- Orthostatic Intolerance (OI)
Orthostatic intolerance (OI) is a medical term covering a group of conditions in which standing upright produces symptoms - dizziness, lightheadedness, racing heartbeat, fatigue, brain fog, and sometimes fainting - that improve once the person sits or lies down, caused by the body's failure to make the rapid cardiovascular and autonomic adjustments needed to keep adequate blood flow to the brain against gravity.
Overview
Understanding Orthostatic Intolerance
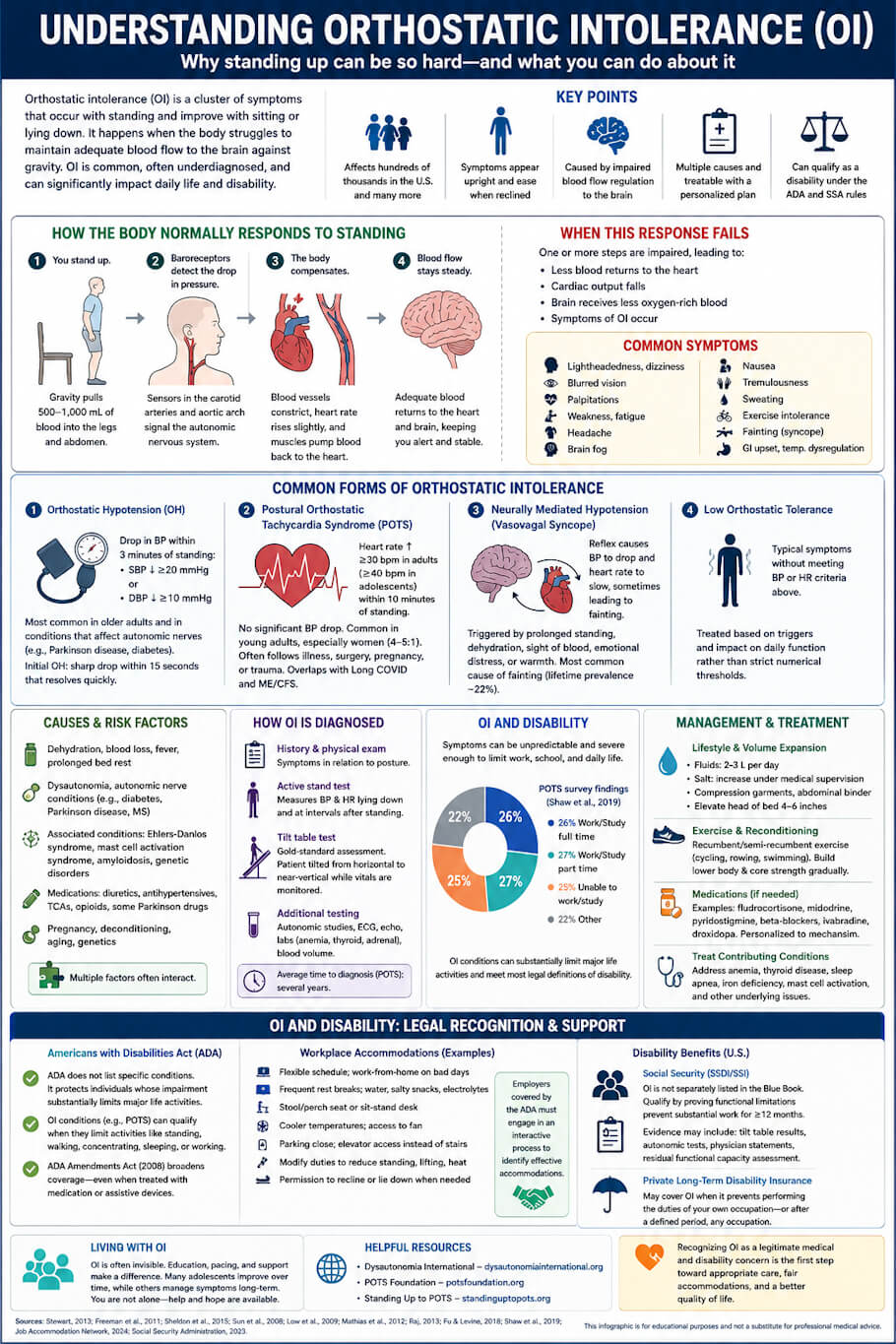
Orthostatic intolerance, often shortened to OI, is a clinical term used to describe a cluster of physical symptoms that develop when a person stands upright and that ease when the person sits or lies down. The word "orthostasis" simply means standing, and OI captures the body's struggle to maintain steady blood flow against gravity once a person is on their feet. While most people rarely think about what happens to circulation during a change in posture, the body must perform a rapid and coordinated set of cardiovascular adjustments every time someone stands. When these adjustments fail or fall short, the brain receives less oxygen-rich blood than it needs, and a recognizable set of symptoms follows.
OI is not a single disease but an umbrella term covering several distinct conditions, including orthostatic hypotension, postural orthostatic tachycardia syndrome (POTS), neurally mediated hypotension, and vasovagal syncope. Researchers estimate that chronic OI affects hundreds of thousands of people in the United States alone, and many more experience milder transient forms during illness, dehydration, or after extended bed rest (Stewart, 2013). Despite its prevalence, OI is frequently underdiagnosed, partly because its symptoms can mimic anxiety, deconditioning, or general fatigue, and partly because routine blood pressure checks taken while seated may miss the problem entirely.
How the Body Normally Responds to Standing
To understand why OI occurs, it helps to picture what happens during a routine stand-up. When a person rises from a seated or lying position, gravity pulls roughly 500 to 1,000 milliliters of blood downward into the abdomen and lower limbs. In a healthy circulatory system, baroreceptors in the carotid arteries and aortic arch detect the drop in pressure within seconds. They signal the autonomic nervous system to constrict blood vessels, increase heart rate slightly, and cue the skeletal and respiratory muscles to pump blood back toward the heart (Stewart, 2013).
This compensatory sequence is so quick that most people never notice it. In someone with OI, however, one or more steps in the sequence is impaired. Blood vessels may not constrict effectively, the heart rate response may overshoot or undershoot, blood volume may be abnormally low, or the autonomic nerves themselves may misfire. The result is that less blood returns to the heart, cardiac output falls, and the brain is briefly under-perfused. Because cerebral blood flow is so closely tied to alertness and balance, even modest reductions can produce noticeable symptoms.
Common Forms of Orthostatic Intolerance
Orthostatic Hypotension
Orthostatic hypotension (OH) is defined as a sustained drop in systolic blood pressure of 20 mmHg or more, or a fall in diastolic pressure of 10 mmHg or more, within three minutes of standing (Freeman et al., 2011). It is most common in older adults and in people with conditions that affect autonomic nerves, including Parkinson disease, diabetes, and multiple system atrophy. Initial orthostatic hypotension, a related variant, produces a sharp pressure drop within 15 seconds of standing and resolves quickly on its own.
Postural Orthostatic Tachycardia Syndrome (POTS)
POTS is characterized by a heart rate increase of at least 30 beats per minute (or 40 beats per minute in adolescents) within 10 minutes of standing, occurring without a significant drop in blood pressure (Sheldon et al., 2015). It tends to affect young adults, with women outnumbering men by roughly four or five to one, and it often follows a viral illness, surgery, pregnancy, or trauma. POTS has received increased clinical attention in recent years because of its overlap with Long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
Neurally Mediated Hypotension and Vasovagal Syncope
Also called neurocardiogenic syncope, this form of OI involves a reflex that causes blood pressure to drop and the heart rate to slow, sometimes producing fainting. Common triggers include prolonged standing, dehydration, the sight of blood, emotional distress, and warm environments. Vasovagal syncope is the most common cause of fainting in the general population, with a lifetime prevalence approaching 22 percent (Sun et al., 2008).
Low Orthostatic Tolerance
Some patients experience the typical orthostatic symptoms without meeting the heart rate or blood pressure criteria for the conditions above. Clinicians sometimes describe this as low orthostatic tolerance and treat it based on the underlying triggers and the impact on daily function rather than on a strict numerical threshold.
Symptoms and How They Present
Symptoms of OI vary widely from one person to the next, but they share a common thread: they appear or worsen with upright posture and ease with reclining. The most frequently reported symptoms include lightheadedness, dizziness, blurred vision, palpitations, weakness, fatigue, headache, brain fog, nausea, tremulousness, sweating, and in more severe cases, syncope (fainting). Many patients also experience exercise intolerance, gastrointestinal upset, and difficulty regulating body temperature (Low et al., 2009).
For example, a college student with POTS might feel fine while sitting in class but become dizzy and short of breath while waiting in line at a cafeteria. An older adult with orthostatic hypotension may rise from a chair, feel the room tilt, and need to sit back down to avoid falling. A teenager with vasovagal syncope might faint after standing in a hot shower or during a long school assembly. The setting changes, but the underlying pattern of upright trigger and recumbent relief stays the same.
Causes and Risk Factors
OI can arise from a wide range of underlying causes. Acute episodes are often linked to dehydration, blood loss, fever, or extended bed rest. Chronic OI, on the other hand, is more likely to involve dysautonomia, an umbrella term for disorders of the autonomic nervous system. Conditions associated with OI include diabetes, Parkinson disease, multiple sclerosis, Ehlers-Danlos syndrome, mast cell activation syndrome, amyloidosis, and several genetic disorders affecting nerve function (Mathias et al., 2012).
Several medications can produce or worsen OI as well, including diuretics, antihypertensives, tricyclic antidepressants, opioids, and some Parkinson drugs. Pregnancy, deconditioning following illness, and aging contribute to risk. Genetics likely plays a role in many cases, since OI conditions sometimes cluster within families. The pathway from cause to symptom is rarely a single line; in most patients, several contributing factors interact at once.
How Orthostatic Intolerance Is Diagnosed
Diagnosis begins with a careful medical history and physical examination, with particular attention to the timing of symptoms in relation to posture. Clinicians often perform an active stand test, in which heart rate and blood pressure are measured while a patient lies down and then again at intervals after standing. The tilt table test, considered a more controlled assessment, involves strapping the patient to a motorized table that gradually shifts from horizontal to nearly vertical while vital signs are continuously monitored.
Additional tests may include autonomic function studies, blood volume measurement, electrocardiography, echocardiography, and laboratory work to rule out anemia, thyroid disease, or adrenal dysfunction. Because symptoms overlap with anxiety disorders and ME/CFS, a thorough evaluation by a physician familiar with autonomic conditions is often necessary to reach a definitive diagnosis (Raj, 2013). Average time from symptom onset to diagnosis remains long, with surveys of POTS patients reporting waits of several years before correct identification (Shaw et al., 2019).
Orthostatic Intolerance and Disability
For many people with OI, the condition is more than an occasional inconvenience. Symptoms can be unpredictable and severe enough to limit education, employment, social participation, and routine self-care. In a large cross-sectional survey of POTS patients, only about a quarter were able to work or study full time, while a similar share reported being too unwell to work at all (Shaw et al., 2019). Chronic fatigue, brain fog, and the risk of falls all contribute to functional limitations that meet most legal definitions of disability.
Functional Limitations
People with OI may struggle with prolonged standing, walking long distances, working in warm environments, climbing stairs, lifting, or sitting upright for extended periods. Cognitive symptoms, often described as brain fog, can affect memory, concentration, and processing speed. Fainting episodes pose a real injury risk, particularly in occupations that involve heights, machinery, or driving. Some patients use mobility aids, including canes, rollators, shower chairs, or wheelchairs, especially during symptom flares.
Legal Recognition Under the Americans with Disabilities Act
The Americans with Disabilities Act (ADA) does not list specific medical conditions. Instead, it defines a person with a disability as someone who has a physical or mental impairment that substantially limits one or more major life activities. OI conditions, including POTS, can meet this definition when symptoms substantially limit activities such as standing, walking, concentrating, sleeping, or working (Job Accommodation Network, 2024). The ADA Amendments Act of 2008 broadened this interpretation to include conditions that remain limiting even when treated with medication or assistive devices, which is particularly relevant for patients who manage symptoms with daily compression garments, salt loading, or pharmacotherapy.
Workplace Accommodations
Reasonable workplace accommodations can help many people with OI remain employed. Common options include:
- Flexible scheduling and the option to work from home on bad days.
- Frequent rest breaks and access to water, salty snacks, and electrolyte drinks at the workstation.
- A stool, perch seat, or sit-stand desk to alternate between postures.
- Cooler ambient temperatures and access to a fan.
- Parking close to the building entrance or use of an elevator instead of stairs.
- Modified duties that reduce prolonged standing, lifting, or work in heat.
- Permission to recline briefly or lie down during a presyncopal episode.
Employers covered by the ADA are required to engage in an interactive process with the employee to identify accommodations that allow the worker to perform essential job functions.
Disability Benefits
In the United States, people with severe OI may apply for Social Security Disability Insurance (SSDI) or Supplemental Security Income (SSI). Although OI is not separately listed in the Social Security Administration's Blue Book, applicants can qualify by demonstrating that their condition causes functional limitations severe enough to prevent substantial work for at least 12 months (Social Security Administration, 2023). Medical evidence typically includes tilt table results, autonomic function tests, treating physician statements, and a residual functional capacity assessment that documents specific limitations on standing, walking, lifting, and concentration. Long-term disability insurance policies may also cover OI when the condition prevents the policyholder from performing the duties of their own occupation or, after a defined period, any occupation.
Management and Treatment
There is no single cure for OI, but a combination of lifestyle measures, physical reconditioning, and medications can substantially reduce symptoms. First-line strategies focus on expanding blood volume and improving venous return. These include increasing fluid intake to two to three liters per day, raising salt intake under medical supervision, wearing compression garments such as waist-high stockings or abdominal binders, and elevating the head of the bed by a few inches.
Graded exercise is a cornerstone of long-term management, particularly for POTS. Recumbent or semi-recumbent exercise, such as cycling, rowing, and swimming, is generally better tolerated than upright walking in the early stages. Strength training of the lower body and core muscles helps the skeletal muscle pump return blood toward the heart and reduces the deconditioning that can perpetuate symptoms (Fu and Levine, 2018).
When lifestyle measures are not enough, clinicians may prescribe medications such as fludrocortisone, midodrine, pyridostigmine, beta-blockers, ivabradine, or droxidopa, depending on the underlying mechanism. Treatment of any contributing condition - thyroid disease, anemia, sleep apnea, iron deficiency, or mast cell activation - is also essential and often improves orthostatic symptoms in parallel.
Living with Orthostatic Intolerance
OI is often invisible to others, which can make daily life particularly difficult. A person who looks healthy may need to sit on the floor of a grocery store, leave a social event early, or pace themselves carefully through a workday. Educating family members, employers, teachers, and clinicians can reduce misunderstandings and improve support. Patient advocacy organizations such as Dysautonomia International, the POTS Foundation, and Standing Up to POTS provide educational resources, peer support groups, and updated research summaries.
For some people, symptoms improve significantly with treatment and time, particularly in adolescent-onset POTS, where many patients see partial or full recovery within several years. For others, OI is a long-term condition that requires ongoing management. In either case, recognizing OI as a legitimate medical and disability concern is the first step toward appropriate care, fair accommodations, and a workable quality of life.
References:
- Freeman, R., Wieling, W., Axelrod, F. B., Benditt, D. G., Benarroch, E., Biaggioni, I., et al. (2011). Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clinical Autonomic Research, 21(2), 69-72.
- Fu, Q., and Levine, B. D. (2018). Exercise and non-pharmacological treatment of POTS. Autonomic Neuroscience, 215, 20-27.
- Job Accommodation Network. (2024). Accommodation and Compliance: Postural Orthostatic Tachycardia Syndrome (POTS). Office of Disability Employment Policy, U.S. Department of Labor.
- Low, P. A., Sandroni, P., Joyner, M., and Shen, W. K. (2009). Postural tachycardia syndrome (POTS). Journal of Cardiovascular Electrophysiology, 20(3), 352-358.
- Mathias, C. J., Low, D. A., Iodice, V., Owens, A. P., Kirbis, M., and Grahame, R. (2012). Postural tachycardia syndrome - current experience and concepts. Nature Reviews Neurology, 8(1), 22-34.
- Raj, S. R. (2013). Postural tachycardia syndrome (POTS). Circulation, 127(23), 2336-2342.
- Shaw, B. H., Stiles, L. E., Bourne, K., Green, E. A., Shibao, C. A., Okamoto, L. E., et al. (2019). The face of postural tachycardia syndrome: insights from a large cross-sectional online community-based survey. Journal of Internal Medicine, 286(4), 438-448.
- Sheldon, R. S., Grubb, B. P., Olshansky, B., Shen, W. K., Calkins, H., Brignole, M., et al. (2015). 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm, 12(6), e41-e63.
- Social Security Administration. (2023). Disability Evaluation Under Social Security (Blue Book). SSA Publication No. 64-039.
- Stewart, J. M. (2013). Common syndromes of orthostatic intolerance. Pediatrics, 131(5), 968-980.
- Sun, B. C., Emond, J. A., and Camargo, C. A. (2008). Direct medical costs of syncope-related hospitalizations in the United States. The American Journal of Cardiology, 95(5), 668-671.
Insights, Analysis, and Developments
Editorial Note: Orthostatic intolerance challenges a basic human capacity, the ability to stand and move freely, and its consequences ripple through work, education, and social life in ways that are easily overlooked by those who do not experience them; understanding the condition and the disability protections that surround it allows patients, families, employers, and clinicians to respond with the recognition and accommodation that decades of autonomic research have long supported.
 Author Credentials: Ian is the founder and Editor-in-Chief of Disabled World, a leading resource for news and information on disability issues. With a global perspective shaped by years of travel and lived experience, Ian is a committed proponent of the Social Model of Disability-a transformative framework developed by disabled activists in the 1970s that emphasizes dismantling societal barriers rather than focusing solely on individual impairments. His work reflects a deep commitment to disability rights, accessibility, and social inclusion. To learn more about Ian's background, expertise, and accomplishments, visit his full biography.
Author Credentials: Ian is the founder and Editor-in-Chief of Disabled World, a leading resource for news and information on disability issues. With a global perspective shaped by years of travel and lived experience, Ian is a committed proponent of the Social Model of Disability-a transformative framework developed by disabled activists in the 1970s that emphasizes dismantling societal barriers rather than focusing solely on individual impairments. His work reflects a deep commitment to disability rights, accessibility, and social inclusion. To learn more about Ian's background, expertise, and accomplishments, visit his full biography.